At the recent American Society of Clinical Oncology annual meeting, a data slide appeared on a screen in a packed convention center hall.
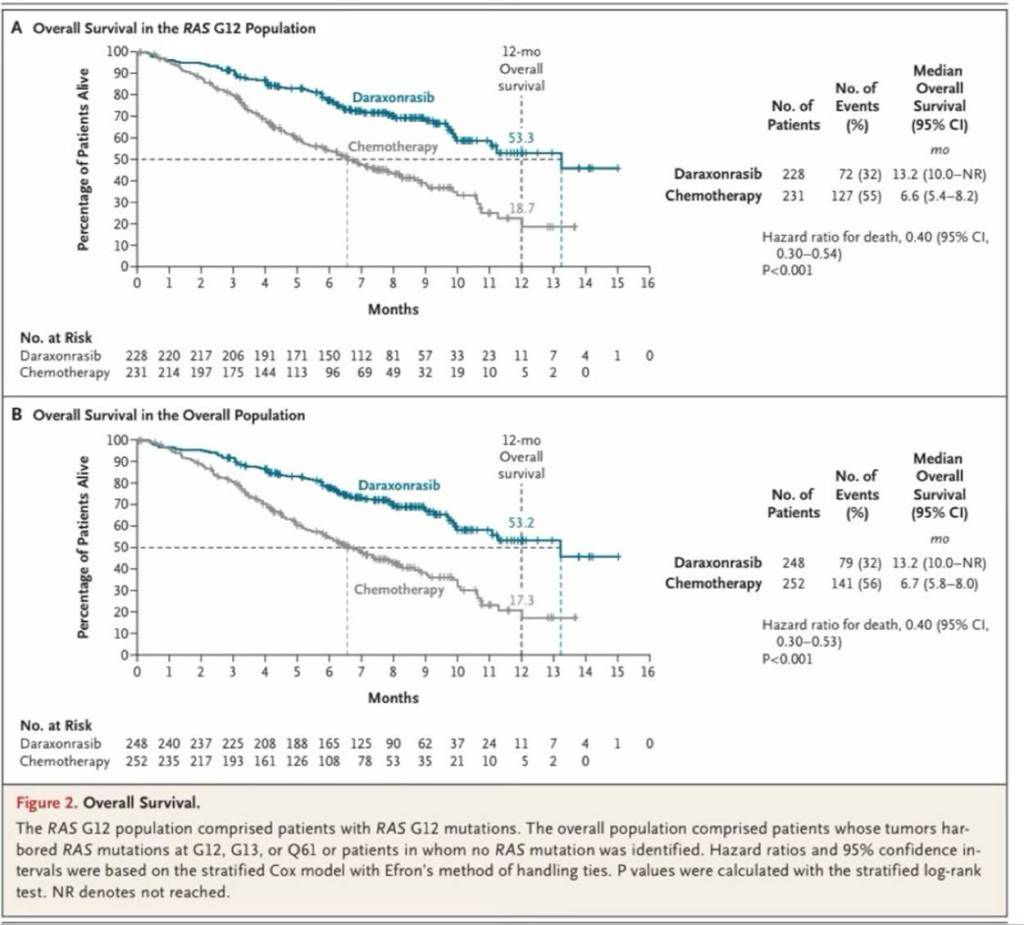
It was a Kaplan-Meier survival curve. Two lines diverging across a graph: one for patients receiving a new drug in combination with chemotherapy, one for patients on chemotherapy alone. This is the kind of visualization oncologists encounter dozens of times a year.
The packed convention center room stood up. Some had tears in their eyes.
The drug was daraxonrasib, developed by Revolution Medicines for patients with RAS-mutated pancreatic cancer. The disease is lethal: just 3% of patients with metastatic pancreatic cancer survive five years after diagnosis. The RAS protein that drives more than 90% of these cancers had been called “undruggable” for decades. Years of attempts failed to effectively target it.
The Phase 3 results: median overall survival of 13.2 months for patients receiving daraxonrasib combined with chemotherapy, compared with 6.7 months for patients on chemotherapy alone. At twelve months, 53% of daraxonrasib patients were alive, compared with 17% of those on chemotherapy. The results were published in the New England Journal of Medicine as the slide projected in the hall. The FDA had already fast-tracked approval and expanded access to patients outside clinical trials made available for free.
Every oncologist attending the meeting already knew the data before it appeared on the screen. The abstract had been published in April. Media had covered the results already. NBC News called it a watershed moment a month before the presentation.
But, knowing what they would see, they stood up anyway.
The question is not what data do we have. It is what does this audience need to see in order to be unable to unsee it.
Evidence That Resolves Rather Than Informs
Emotional connection without evidence is anecdote. Evidence without emotional connection is noise. The discipline is knowing when to lead with which, and how to integrate them so that momentum builds.
What made the daraxonrasib curve move a room full of stoic clinicians? Not novelty. The audience already knew the numbers. What moved them was context. The decades of failure that preceded it. The patients who had run out of options. The science that had finally worked where every previous attempt had not.
The data did not arrive in a vacuum. It arrived at the conclusion of an argument the entire field had been making for years. When that survival curves appeared on the screen, it resolved the argument rather than simply restating it. There was nothing left to interpret.
That is what precision in science presentation achieves. Not performance. Resolution.
Evidence That Performs vs. Evidence That Persuades
Most organizational communications deploy evidence the way convention centers deploy signage: to mark the territory, not to move anyone through it.
A company announces a milestone and includes a market size figure because the number is large. A clinical team presents a dataset and adds three supplementary datasets for comprehensiveness. A policy argument is made and citations are appended below it. The evidence is present. The argument never arrives.
Engagement by Design embraces evidence-based communications, but the discipline is not about volume. It is about selection. Every claim anchored. Every certainty level calibrated. Every data point chosen because it advances the argument rather than decorates it. It is coordinated narrative arc delivering an experience that is quite like an opera. The integration of multiple arts strategically designed to produce a magnificent, impactful experience. Narrative and data points that spark excitement all over the brain.
For the oncologists at ASCO, the right evidence was two lines on a graph. Demonstrably separated from month one. Thirteen months survival versus seven. Fifty-three percent versus seventeen as twelve months. And the weight of everything that had been tried before. The room filled with careers understanding why those numbers were impossible. The curves included in the accompanying NEJM publication will tell the story for many years to come:
Credibility That Compounds
There is a longer argument for strategic science and evidence-based communication that extends beyond any single presentation.
Stakeholders who trust your evidence base return to you when the stakes are highest. The organization that has shown it understands certainty levels, that it does not overstate, that it acknowledges what is not yet known, that it chooses specificity over impressiveness, builds credibility that compounds over time. It is not simply believed in the moment. It is the first call when the next decision needs to be made.
The inverse is equally true. An organization that reaches for evidence that performs, that selects data for its size rather than its relevance, that adds citations without regard to the context, teaches its audience to discount what it says. That discount applies to every future communication.
The ASCO debut was the culmination of years of rigorous science and clinical development, each stage held to the same standard: show what is true, show what it means, show what it changes. By the time the slide appeared, the room was prepared to believe it.
That preparation is the work.
The Question to Ask Before the Next Data Communication
The Impact Imperative returns to the same standard across every episode: does your engagement strategy produce evidence of impact, or only evidence of effort?
For evidence-based engagement, the questions are direct. Does each data point advance the argument, or does it simply occupy space? Has the evidence been chosen from the audience’s frame of reference, what they already know, what they have been unable to solve, what failure looked like before? Could a person in your audience reconstruct the argument from the evidence alone?
If the honest answer leans toward decoration, the left brain has been left out of the room.
That is where our work together begins.
